BACKGROUND PAPER
June 2016
Click here for a PDF of this backgrounder complete with references
SUMMARY
Anosognosia is an awkward term introduced by neurologists a century ago to denote “a complete or partial lack of awareness of different neurological . . . and/or cognitive dysfunctions.” It is not the same as denial of illness. Anosognosia is caused by physical damage to the brain, and is thus anatomical in origin; denial is psychological in origin.
The late, eminent neurologist Oliver Sacks described anosognosia thus:
It is not only difficult, it is impossible for patients with certain right-hemisphere syndromes to know their own problems – a peculiar and specific ‘anosognosia,’ as Babinski called it. And it is singularly difficult, for even the most sensitive observer, to picture the inner state; the ‘situation’ of such patients, for this is almost unimaginably remote from anything he himself has ever known.
Approximately 50% of individuals with schizophrenia and 40% of individuals with bipolar disorder are estimated to have co-occurring anosognosia. It is reported to be the most common reason why individuals with schizophrenia refuse to take medication; since they do not believe that there is anything wrong with them, why should they? Awareness of illness sometimes improves with treatment with antipsychotic medication, especially clozapine.
BACKGROUND
Among neurological patients, anosognosia is seen most commonly in Alzheimer’s disease, Huntington’s disease and traumatic brain injury. Most patients with Alzheimer’s disease, for example, are aware that something is wrong early in the course of their illness but then lose all awareness of their illness as it progresses. Anosognosia is seen less commonly in patients with stroke (especially those involving the right parietal lobe) and Parkinson’s disease. Impaired awareness of illness is not a new idea for psychiatric patients either; in 1604, a character in playwright Thomas Dekker’s The Honest Whore says, “That proves you mad because you know it not.”
ANOSOGNOSIA RESEARCH SUMMARIZED
Since 1992, there have been 22 studies comparing the brains of individuals with schizophrenia with and without anosognosia. In all but two studies, significant differences are reported in one or more anatomical structures. Since anosognosia involves a broad brain network concerned with self-awareness, a variety of anatomical structures are involved, especially the anterior insula, anterior cingulate cortex, medial frontal cortex, and inferior parietal cortex. Three of the positive studies included individuals with schizophrenia who had never been treated with medications, discounting the likelihood that the observed brain changes resulted from treatment.
Earlier anosognosia research is summarized by Xavier Amador, PhD, and Tony David in their 2004 book, Insight and Psychosis: Awareness of Illness in Schizophrenia and Related Disorders.
Following is a summary of 25 studies of anosognosia in psychiatric disease, beginning from the most recent.
- Awareness of illness found associated with thickness of insula cortex.
In Canada, researchers at McGill University used magnetic resonance imaging (MRI) to assess 66 individuals with chronic schizophrenia and 33 healthy controls. The Scale to Assess Insight (SAI-E) was used to assess insight into symptoms. Patients with low awareness of symptoms had significantly thinner right insula cortex. The insula is increasingly thought to be a key structure for self-perception. - Awareness of illness found associated with brain connectivity.
In Canada, Gerretsen and colleagues at the University of Toronto studied the association of awareness of illness to brain connectivity. Twenty individuals with schizophrenia were assessed for clinical and cognitive insight using SAI-E. Individuals with impaired insight on resting MRI showed increased connectivity in the default mode network in the left angular gyrus and in the self-referential network in the left insula. - Awareness of illness found associated with changes in the brain that can be seen microscopically.
At the Mental Health Research Center in Moscow, sections of the brain from 24 deceased individuals with schizophrenia were examined microscopically. This was the first study to study the brains of people who died with schizophrenia under microscope and to include individuals with and without symptoms of anosognosia. Two brain areas known to be important in anosognosia were assessed: (1) supramarginal and angular gyri and (2) BA 40 and 39 of the inferior parietal lobule. The 24 individuals were assessed postmortem for awareness of illness by examining their medical records for explicit denial of illness; refusal to take medication; and/or failure to follow treatment plans. Among the 24, 9 were found to have had good awareness and 15 “fair” or “poor” awareness of illness.
In the brains of individuals with fair or poor insight, a 21% reduction in glial cells was found (specifically obligodendroglia). These brains differed statistically from the normal control brains (p=0.04) and, at the borderline, and from those without anosognosia (p=0.055). The brains of the individuals without anosognosia (good insight) did not differ from the normal controls. Those with anosognosia additionally had fewer glial (obligodendroglial) cells. - Awareness of illness found associated with hemispheric asymmetry in schizophrenia.
In Canada at the University of Toronto, 52 individuals with schizophrenia were assessed for awareness of illness (using the relevant item on the Positive and Negative Syndrome Scale (PANSS)) and underwent MRI.
Lack of awareness of illness (anosognosia) was strongly correlated with both severity of illness (p<0.01) and with total white matter volume (p<0.01). Hemispheric asymmetry was evident with the right hemisphere showing less volume than the left hemisphere in patients with impaired awareness of illness, specifically in the anterior end of the inferior temporal lobe (p=0.05); the dorsal lateral prefrontal cortex (p=0.003); and the inferior parietal lobe (angular gyrus) (p=0.05). These findings are consistent with the occurrence of anosognosia in some individuals when stroke occurs in the right hemisphere and suggests that awareness of illness in schizophrenia is likely more associated with to the right hemisphere than to the left.
The authors of the study noted that persons with schizophrenia vary in their degree of anosognosia: “They can have equally bizarre delusions or perceptual disturbances but can be quite dissimilar in their ability to recognize that these experiences arise from their mind rather than a part of objective reality.” This combination of insight with profound mental disturbances is one of the most puzzling aspects of schizophrenia for family members. - Awareness of illness found associated with the function of the medial prefrontal cortex, insula and inferior parietal lobule.
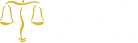
In the Netherlands, 47 individuals with schizophrenia and 21 normal controls were assessed by functional MRI (fMRI). They were asked to perform tasks that required them to think about themselves (self-reflection) while their brains were being scanned.
Individuals with anosognosia (i.e., with less ability to think about themselves) showed significantly poorer activation in several brain areas, including parts of the frontal and parietal lobes. These were statistical differences at the group level but cannot yet be used to predict anosognosia in any given individual.
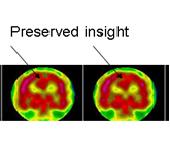
The following pictures illustrate the differences. Scanned from one individual with schizophrenia who has good insight (high self-reflection) and a second with poor insight (low self-reflection), significantly better activation in the insula and the inferior parietal lobule (IPL) are observed in the individual with good insight (see Figure 1). Figure 2 shows much better activation in the medial prefrontal cortex (MPFC) in the individual with good insight.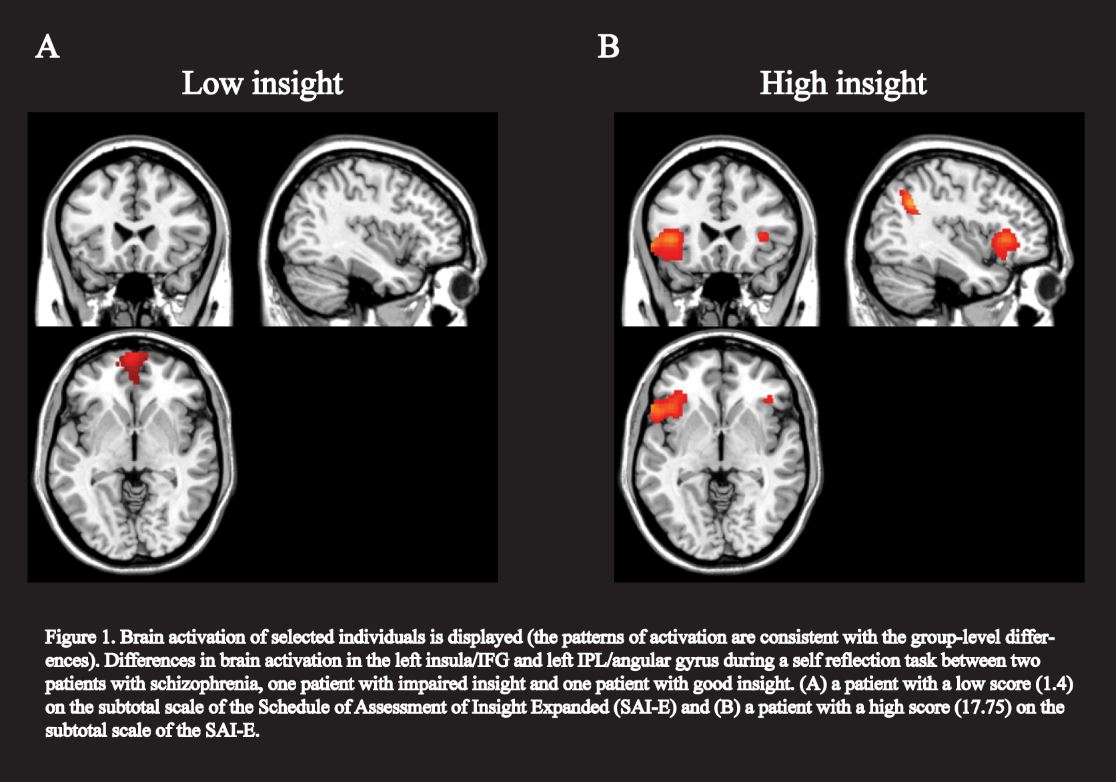
- Awareness of illness found associated with the function of midline brain structures.
In Finland, 21 patients with schizophrenia and 17 normal controls underwent both structural magnetic resonance imaging and fMRI, during which time they were asked to answer specific questions about insight (e.g., “If someone said I had a mental illness, they would be right”). Insight was associated with activation of brain midline structure, specifically posterior cingulate, medial prefrontal cortex and frontal pole, brain areas known to be associated with self-awareness. The authors acknowledged that “the present findings . . . cover only a portion of the neuronal circuitries involved in the processing of insight.” - Anosognosia found associated with impaired cerebral blood flow in the superior parietal area (precuneus).
In France, 31 patients with paranoid schizophrenia and 18 normal controls were assessed for cerebral blood flow by single photon emission computed tomography. Twenty-one patients were deemed to have good awareness of their illness and 10 were not. Those with poor awareness of illness showed poor cerebral blood flow bilaterally to the precuneus (p<0.001), a part of the superior parietal lobe known to be involved in self-consciousness, including awareness of one’s own emotional state. There were no differences in the frontal lobes (see Figure 3).
- Anosognosia found associated with a decrease in gray matter.
In Spain, 21 individuals with first-episode schizophrenia and who had never been treated were compared on MRI with 20 controls. Three items from the Scale to assess Unawareness in Mental Disorder (SUMD) were used to assess insight. Patients with poorer insight had a significant decrease in gray matter volume in medial superior frontal gyrus, inferior frontal gyrus, inferior temporal gyrus, and cerebellum. - Anosognosia found associated with widespread impairments in white matter.
At New York University, 36 individuals with schizophrenia and schizoaffective disorder underwent diffusion tensor imaging (DTI), which assesses brain white matter integrity. Those with poorer awareness of illness were significantly more likely to have impaired white matter function in the frontal lobe (e.g., left middle and right superior frontal gyri); temporal lobe (e.g., bilateral parahippocampal gyri); cingulate; thalamus; and basal ganglia (caudate and lentiform nucleous). - Anosognosia found associated with decreased cortical thickness.
In Montreal 79 individuals with first-episode psychosis were assessed clinically and by MRI. Poorer awareness of illness was significantly associated with having a thinner brain cortical layer in the left middle frontal gyrus, left inferior frontal gyrus, left inferior temporal gyrus, left and right precentral gyrus, and right occipital gyrus. Impaired awareness of need for treatment was significantly associated with a thinner brain cortical layer in the left middle and medial frontal gyri; parietal precuneus and supramarginal gyrus; temporal parahippocampus and superior, middle and inferior gyri; and middle occipital gyrus. The authors concluded that “insight involves a network of brain structures, and not only the frontal lobes as previously suggested.” - Anosognosia found associated with impairments in midline brain structures (posterior cingulate and precuneus).
In England, 82 individuals with first episode psychosis and 91 normal controls were assessed on neuropsychological tests and by MRI. 20 of the individuals with first episode psychosis “had no capacity to identify psychotic symptoms as pathological.” Compared with the other 62 individuals, those 20 had “significantly reduced global gray matter volume,” most marked in the left posterior cingulate cortex, the right precuneus, and the cuneus. - Anosognosia found associated with impairments of temporal and parietal areas.
In England, 52 individuals with schizophrenia or schizoaffective disorder and 30 normal controls were assessed for awareness of symptoms and underwent MRI. Those with poorer awareness of their symptoms had decreased gray matter volume in their left superior, left middle and right inferior temporal gyri, as well as in the right inferior parietal lobule and right supramarginal gyrus (all p<0.001). - Anosognosia found associated with decreased gray matter volume of the prefrontal cortex.
In England, 28 outpatients with stable schizophrenia were assessed for insight and underwent MRI. Lower levels of insight were moderately associated with decreased volume of the prefrontal gray matter, especially the inferior frontal gyrus. - No association found between anosognosia and regional brain volumes.
In Italy, 50 patients with schizophrenia and 30 normal controls were assessed for awareness of illness and by MRI. No relationship was found between awareness of illness and the gray and white matter volumes in the frontal or temporal cortex. - Anosognosia found associated with decreased activation of the left medial prefrontal cortex.
In England, 14 individuals with schizophrenia were subjected to fMRI both during an acute schizophrenia episode and again after they had been stabilized. During their fMRI, they were asked to do tasks which measured social functioning and awareness of illness. Their left medial prefrontal cortex showed improved activation when they were stabilized, and this correlated with improvement in insight scores (r=0.81, p<0.001). - Anosognosia is associated with decreased gray and white matter.
At multiple sites in the United States and Europe, 251 individuals with first-episode psychosis were assessed for awareness of illness, using the Insight and Treatment Attitude Questionnaire (ITAQ), and for brain volume, using MRI. Decreased whole brain volume, whole brain gray volume, and whole brain white volume were all statistically associated with decreased awareness of illness. - Anosognosia found associated with decreased volume of right dorsolateral prefrontal cortex and right orbitofrontal cortex.
At the University of Texas Southwestern, 14 patients with schizophrenia and 21 normal controls were assessed for awareness of illness and symptoms and by MRI. Patients with poorer awareness of illness and symptoms also had significantly smaller right dorsolateral prefrontal cortex (r= -0.72, p= 0.04). - Anosognosia found associated with reduced gray matter in the cingulate and inferior temporal regions.
In South Korea, 35 patients with paranoid schizophrenia and 35 matched normal controls underwent clinical testing and MRI. Those with greater “lack of judgment and insight” had reduced gray matter in their right anterior cingulate, left posterior cingulate and inferior temporal region on both sides. - Anosognosia found associated with decreased volume of the right dorsolateral prefrontal cortex.
At the University of Pittsburgh, 35 individuals with first episode schizophrenia, none of who had been treated with any antipsychotic drugs, were assessed clinically, neuropsychologically and by MRI of the frontal lobes and hippocampus. Eighteen patients had poor awareness of their illness and 17 had good awareness. Those with poor awareness were found to have decreased volumes of their right dorsolateral prefrontal cortex (DLPFC) (r= -61, p = 0.008). Unawareness of illness was not associated with hippocampal volume, duration of illness or other clinical symptoms. - Anosognosia found not correlated with global brain measures.
In England, 78 men with schizophrenia and 36 normal controls were assessed for awareness of illness and underwent MRI. There were “no significant correlations between total insight score and grey, white, CSF and total brain volume.” The authors concluded that such research was not likely to be useful for such “global brain measures” and that “future investigations should pay attention to more specific cortical regions.” - Anosognosia found associated with specific subregions of the frontal lobes.
At Dartmouth Medical School, 15 individuals with schizophrenia and schizoaffective disorder were assessed for awareness of illness and frontal brain structures by MRI. Those with less awareness of their illness had significantly smaller bilateral middle frontal gyrus volume (r= -0.92 and -0.72, p<0.01) than those with more awareness. There was also a trend for individuals with poor awareness to have a smaller right gyrus rectus and left anterior cingulate gyrus. The authors concluded that “the strong correlations between bilateral middle frontal gyri and unawareness suggest involvement of dorsolateral prefrontal cortex,” an area that has been associated with schizophrenia in many neuropsychological and neuropathological studies. - Anosognosia found associated with atrophy of the frontal lobes.
In Norway, 21 individuals with schizophrenia and 21 matched normal controls were assessed by computerized tomography (CT) scans. Seven of the 21 individuals with schizophrenia showed mild or moderate atrophy of their frontal lobes, and this atrophy correlated with poorer awareness of illness (r= -0.52, p<0.05). Poorer awareness of illness also correlated with poorer executive function, a frontal lobe-associated trait, but not with other neuropsychological measures. The authors concluded that “unawareness of illness in schizophrenia may be related to frontal lobe deficit.” - Anosognosia found associated with having a smaller brain size.
At Dartmouth Medical School, 18 individuals with schizophrenia and a poor awareness of their illness were compared on MRI with 12 individuals with schizophrenia and a good awareness of their illness and with13 healthy controls. There were no differences between the schizophrenia groups on education, symptoms or severity of illness. However, those with poor awareness of their illness were found to have significantly smaller brains and decreased intracranial volumes, findings consistent with a loss of brain tissue (atrophy) associated with schizophrenia. - Anosognosia does not correlate with total ventricular volume.
In England, 128 individuals with recent-onset psychosis were assessed for awareness of illness and underwent a computerized tomography (CT) scan. No correlation was found between awareness of illness and total ventricular volume. - Anosognosia correlates with enlarged brain ventricles.
In Japan, 22 patients with chronic schizophrenia were assessed for awareness of illness and underwent MRI. Those patients with impaired awareness of illness had significant ventricular enlargement (p<0.05).